


Did you know?
Your patients' physical well-being depends on their psychological well-being.
(Of course you did. But to this extent?)
Did you know?
Most of your patients are convinced of the mind-body connection.
Did you know?
Most of your patients would be readily referred to a psychologist.
Did you know?
Most of your patients benefit and feel better after therapy.
(The right therapist, of course.)
Did you know?
Cognitive Therapy is an effective treatment for depression and anxiety.
(You probably knew this.)
But did you also know?
Cognitive Therapy may be superior to antidepressant medication.
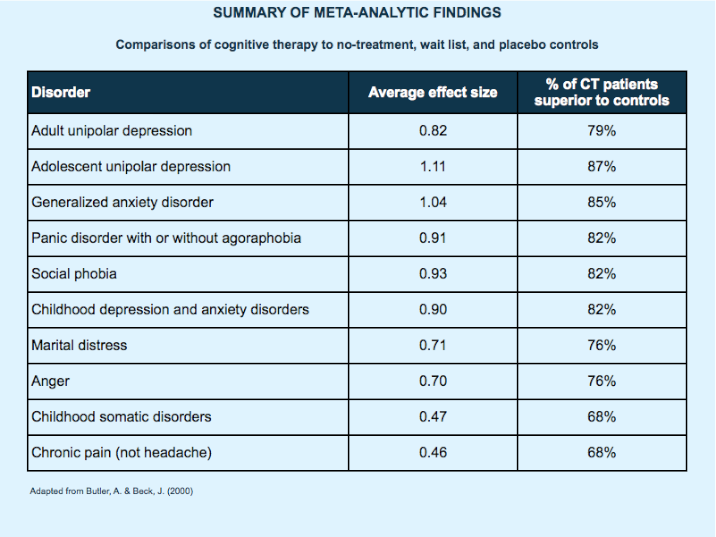
Butler, A. C., & Beck, J. S. (2000). Cognitive therapy outcomes: A review of meta-analyses. Journal of the Norwegian Psychological Association, 37, 1-9.
"How effective is cognitive therapy (CT), for which disorders, and compared to what? To answer this question, we review 14 recent meta-analyses that investigate the efficacy of CT. These meta-analyses covered collectively 9,138 subjects in 325 studies and involved 465 comparisons regarding 14 disorders or populations. Findings indicate that CT is substantially superior to no-treatment, wait list, and placebo controls for adult and adolescent unipolar depression, generalized anxiety disorder, panic disorder with or without agoraphobia, social phobia, and childhood depressive and anxiety disorders. The effect sizes for these comparisons (M = 0.90, SD = 0.07) were large by Cohen's (1988) criteria. Corresponding effect sizes for CT of marital distress, anger, childhood somatic disorders, and chronic pain were in the moderate range (M = 0.62, SD = 0.11).
"CT was somewhat superior to antidepressants (ES = 0.38) in the treatment of adult depression. A year after treatment discontinuation, depressed patients who had been treated with CT had half the relapse rate of depressed patients who had been treated with antidepressant medication. CT was equally effective as behavior therapy in the treatment of adult depression (ES = 0.05) and obsessive-compulsive disorder (ES = .19). In the small number of direct comparisons of CT with supportive/nondirective therapy – two for adolescent depression and two for generalized anxiety disorder– CT was superior (M = 0.77, SD = 0.25). CT was somewhat superior to a group of miscellaneous psychosocial treatments for sexual offending (ES = 0.35). Although controlled meta-analyses are lacking for CT of bulimia nervosa, large effect sizes have been obtained for pre-to-posttreatment improvement (M = 1.27, SD = 0.11). "
"What is an effect size?
Effect sizes of the type we report here represent the difference between two group outcomes in standard deviation units. Hence, an effect size of 0 would indicate no difference between group outcomes, whereas an effect size of 0.50 would indicate that the outcome of the cognitive therapy group was one-half a standard deviation larger (better) than the outcome of the control group. An effect size of 1.0 (a one-standard-deviation difference) is large and would indicate that the average cognitive therapy patient had an outcome superior to that of 84% of the control group. Effect sizes have been categorized along a continuum of no effect (0 to 0.2), low effect (0.2 to 0.5), medium effect (0.5 to 0.8) and high effect (greater than 0.8)."
Did you know?
The American Academy of Family Physicians Recognizes:
Cognitive Therapy is an effective treatment for depression.
(You may have known this.)
But did you also know?
Cognitive Therapy is as effective and possibly more effective than pharmacotherapy in managing mild to moderate unipolar depression.
Rupke, S.J., Blecke, D., & Renfrow, M. (2006). Cognitive therapy for depression. American Family Physician, 73:83-6,
"Numerous studies and meta-analyses demonstrate convincingly that cognitive therapy or CBT effectively treats patients with unipolar major depression. Several studies have shown that cognitive therapy is superior to no treatment or to placebo. Two comprehensive meta-analyses showed that cognitive therapy is as effective as interpersonal or brief psychodynamic therapy in managing depression. They also showed that cognitive therapy is as effective and possibly more effective than pharmacotherapy in managing mild to moderate unipolar depression.
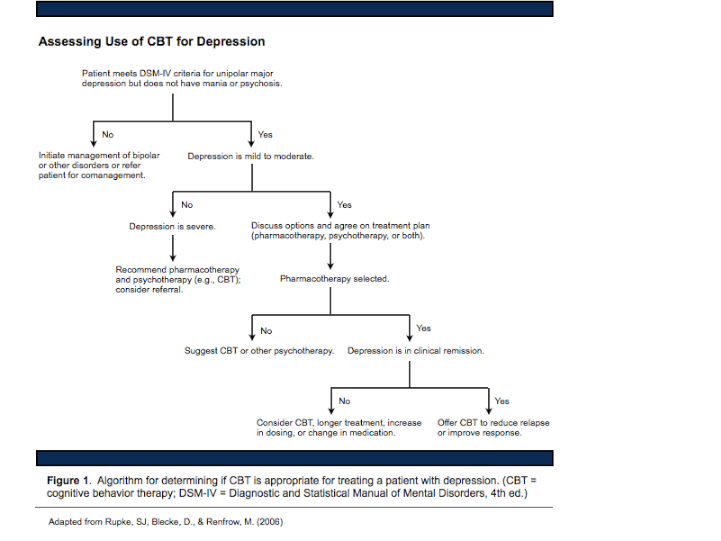
"The National Institute of Mental Health Treatment of Depression Collaborative Research Program compared the effectiveness of two forms of psychotherapy (i.e., interpersonal therapy and CBT) with imipramine (Tofranil) or placebo in the treatment of 250 patients with major depressive disorder. The study found no significant differences between the therapies; however, the two psychotherapies were slightly less effective than imipramine but more effective than placebo. A meta-analysis of four studies, which included 169 patients with major depression, showed similar results for tricyclic antidepressants and CBT. The evidence suggests that cognitive therapy is a valid alternative to antidepressants for patients with mild to moderate depression and possibly for patients with more severe depression. Figure 1 is an algorithm for determining if CBT is appropriate.
". . . Family physicians usually are the first to diagnose and treat patients with depression. They should inform patients that psychotherapy and pharmacotherapy are valid options, and that cognitive therapy, and therefore CBT, is the most studied psychotherapy. If the patient and physician initially elect to use pharmacotherapy, and the patient does not respond adequately, the physician should again suggest adding psychotherapy or CBT. CBT should be strongly considered as initial therapy for patients with severe or chronic depression or for adolescents."
Did you know?
Ponte Vedra Psychologist Dr. Gregory Garamoni specializes in Cognitive Therapy
Call 285-4229 for an appointment![]()
Back to the top